ghost content

What is Graves’ Disease?
Graves’ disease is an immune system disorder that results in the overproduction of thyroid hormones (hyperthyroidism).
Named for Sir Robert Graves (1796-1853), Graves’ disease is the most common cause of hyperthyroidism.
Graves’ is an autoimmune disease and not necessarily a thyroid disease. With an autoimmune disorder, such as Graves’ disease, your immune system mistakenly turns against your body.
With Graves’ disease, the antibodies your body produces are against the receptors on your thyroid causing your metabolism to speed up.

The Most Common Autoimmune Disorder in the United States

3 MILLION
PEOPLE IN THE U.S.
12,000
CASES PER MONTH
8:1
WOMEN TO MEN
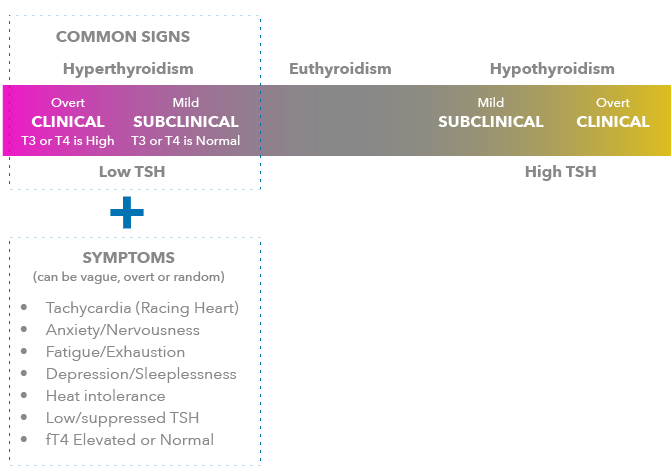
Low TSH and symptoms usually begin the investigation
For unknown reasons your immune system creates antibodies called thyroid-stimulating immunoglobulins (TSIs). These antibodies cause your thyroid gland to produce more thyroid hormone than your body needs.
The TSIs fool the thyroid gland into over-producing thyroid hormone, which causes hyperthyroidism.
Family history and gender may also be factors.
Effects of TSI
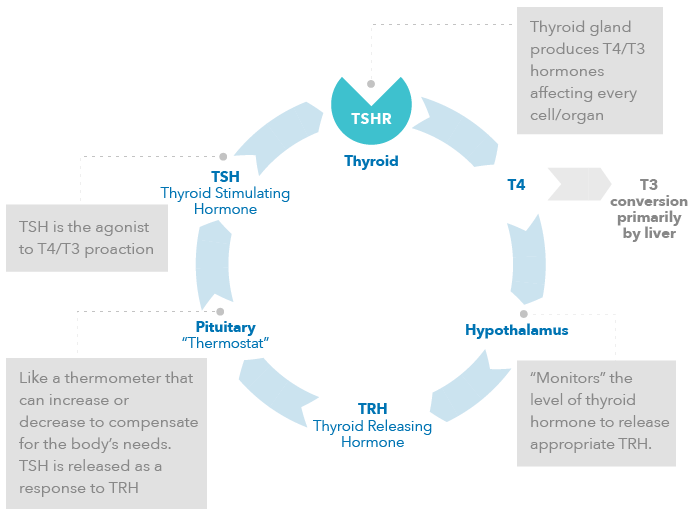
In normal thyroid metabolism, thyroid hormone production is tightly regulated by the hypothalamic-pituitary-thyroid axis. The pituitary gland releases Thyroid Stimulating Hormone (TSH) in response to thyroid releasing hormone (TRH) from the hypothalamus, which monitors T4 and T3 levels in the blood stream. TSH binds to its receptor on the thyroid gland and stimulates production and release of T4 and T3. If T4 and T3 levels fluctuate outside of a normal range, TSH production is increased or lowered to compensate.
NORMAL THYROID FUNCTION
Negative feedback loop
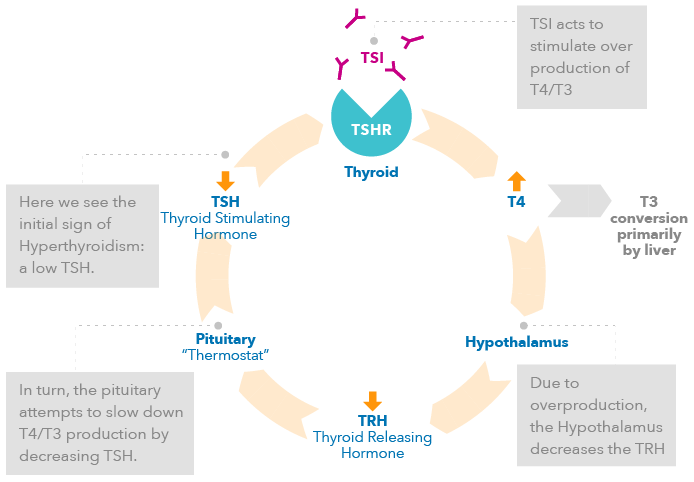
Thyroid Stimulating Immunoglobulin (TSI) mimics the action of TSH on the thyroid gland in that it causes T4 to be over produced, but TSI is not regulated by the same negative feedback system. As a result TSI continues to stimulate the thyroid even after hormone levels are elevated, leading to an overabundance of hormones, and thus hyperthyroidism.
EFFECTS OF TSI – PATIENTS WITH GRAVES’ DISEASE
TSI antibodies can pass through the placenta and affect the fetus. As a result, the ATA/AACE issued the following guidance:
- Recommendation 74: TSH receptor (TSH-R) antibody levels should be measured to differentiate the etiology of hyperthyroidism in pregnancy
- Recommendation 75: Patients who were treated for Graves’ disease prior to pregnancy should have TSH-R antibody levels initially during the first trimester and, if elevated, again at 22-26 weeks of gestation
- Recommendation 76: Patients diagnosed with Graves’ disease during pregnancy should have TSH-R antibody levels measured at diagnosis and again at 22-26 weeks of gestation
- Recommendation 77: TSH-R antibody levels measured at 22-26 wks of gestation should be used to guide decisions regarding neonatal monitoring
The American Thyroid Association recommends that the following high-risk women be screened for thyroid disease either prior to becoming pregnant, or as soon as feasible once a woman becomes pregnant:
- Women with a history of thyroid disease or thyroid surgery.
- Women with a family history of thyroid disease
- Women with a goiter
- Women with known thyroid antibodies
- Women with symptoms or clinical signs of hyperthyroidism or hypothyroidism
- Women with Type I diabetes mellitus
- Women with other autoimmune disorders
- Women with infertility
- Women with previous therapeutic head or neck irradiation
- Women with a history of miscarriage or preterm delivery

How can Thyretain help?
Thyretain TSI Reporter BioAssay detects TSI, the causative agent of Graves’ disease, in patient serum. Other thyroid receptor antibody (TRAb) assays are nonspecific in that they cannot differentiate between blocking, binding and stimulating antibodies (immunoglobulins). Based on a novel genetically engineered cell line, Thyretain detects only stimulating immunoglobulins. The engineered cell technology also enhances the sensitivity for detecting TSI , providing improved results over currently available non-specific assays.
Thyretain Can Quickly Help Differentiate Graves’ Disease Induced Autoimmune Hyperthroidism from Non-Autoimmune Hyperthroidism
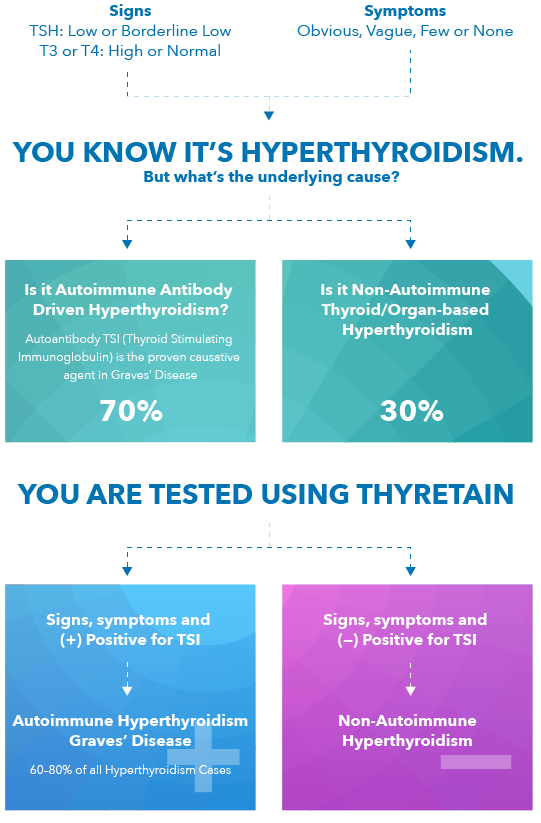
- TSI is the autoantibody that stimulates TSH receptors – and is the cause of Graves’ Disease. 1
- Quidel’s TSI Reporter Assay (Thyretain) is the only FDA-cleared bioassay that specifically identifies TSI.
- If a positive TSI result, patient has autoimmune disease; a differential diagnosis of Graves’ can be confirmed. 1,2
The assay is a living system and responds as your body would to TSI.The genetically engineered cell line in Thyretain has a version of the TSH receptor that is naturally found on your own thyroid. When test serum is allowed to incubate with these cells any TSI binds to this receptor and a cyclic AMP triggers the production of firefly luciferase. Just like fireflies you might see flashing light on a summer evening, the cells emit light that can then be detected using a special device.

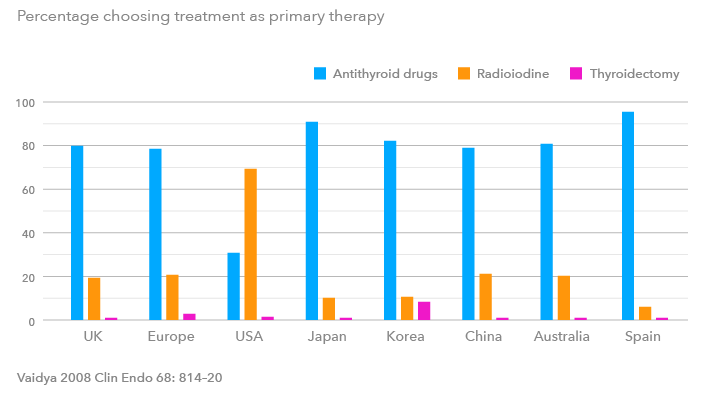
(Treatment is a personal choice and Quidel does not advocate one therapy over another)
Medical Management Therapy
Antithyroid drugs (ATD) are suppressive drugs meant to inhibit the production of thyroid hormones T4 and/or T3 in an effort to treat the symptoms of Graves’ disease. These medications include Methimazole (MMI), and propylthiouracil (PTU). MMI and PTU act by inhibiting the synthesis (the production) of thyroid hormone. PTU use has been stopped especially in children, due to effects on liver function. MMI is widely used and does not carry this restriction. Medical management has a success rate of ~45-50% using current medical management guidelines. Patients retain their thyroid and may have remission of the autoimmune response. Those patients who do not respond to the ATD therapy can either continue the ATD or chose the definitive cure options listed below.
There are some side effects when using ATDs that can occur. Most are mild (rash occurs in 3-4% of patients), but one in particular is severe (agranulocytosis occurs in ~0.3% of patients). This is extremely rare and corrected by stopping the ATD therapy.
DEFINITIVE THERAPIES
Radioiodine Ablation Therapy
Iodine-131 (Radioiodine) is given orally to destroy the function of a hyperactive gland. Usually one dose is sufficient but some patients might require more than one treatment. The radioactive iodine is picked up by the active cells in the thyroid, which use iodine to produce T4, and destroys these cells.
Radioiodine is an ablative approach and is considered the definitive cure for hyperthyroidism brought about by eliminating most if not all of the target organ; however, >80% of patients develop permanent hypothyroidism soon after treatment and require lifelong synthetic hormone replacement. Hypothyroidism is believed to be an easier disease to manage than hyperthyroidism.
Theoretically the radioiodine could be dosed to only destroy part of the thyroid gland, but the dosage is extremely difficult to determine, and if thyroid tissue remains, the body can still produce TSI against any remnant tissue. These antibodies can still cause Graves’ eye disease even after ablative therapy. For incompletely ablated women in their child bearing years these antibodies could be passed across the placenta during pregnancy, leading to the child developing Graves’ disease. This has been addressed in the ATA and AACE guidelines for treating patients with a history of thyroid disease in pregnant women and those considering pregnancy who have undergone this treatment. (see Graves’ disease and Pregnancy)
Surgery
This option is also considered a definitive cure for Graves’ disease. For patients who cannot tolerate medicines or who are allergic to or decline iodine-131, a surgical treatment option is available. Full or partial thyroidectomy is used uncommonly in the US and is not considered a primary option for Graves’ disease treatment, due to risks from surgery and anesthesia. If this option is chosen, it is important to select a surgeon with sufficient skill in thyroid surgery specifically.
*References
TREATMENT CAN VARY BY REGION
Percentage choosing treatment as primary therapy